For more than three decades, billing an obstetric pregnancy in the United States has been almost surgically simple: one global code — most commonly CPT 59400 — covered every prenatal visit, the delivery itself, and routine postpartum care, all paid as a single bundled fee. That model is ending.
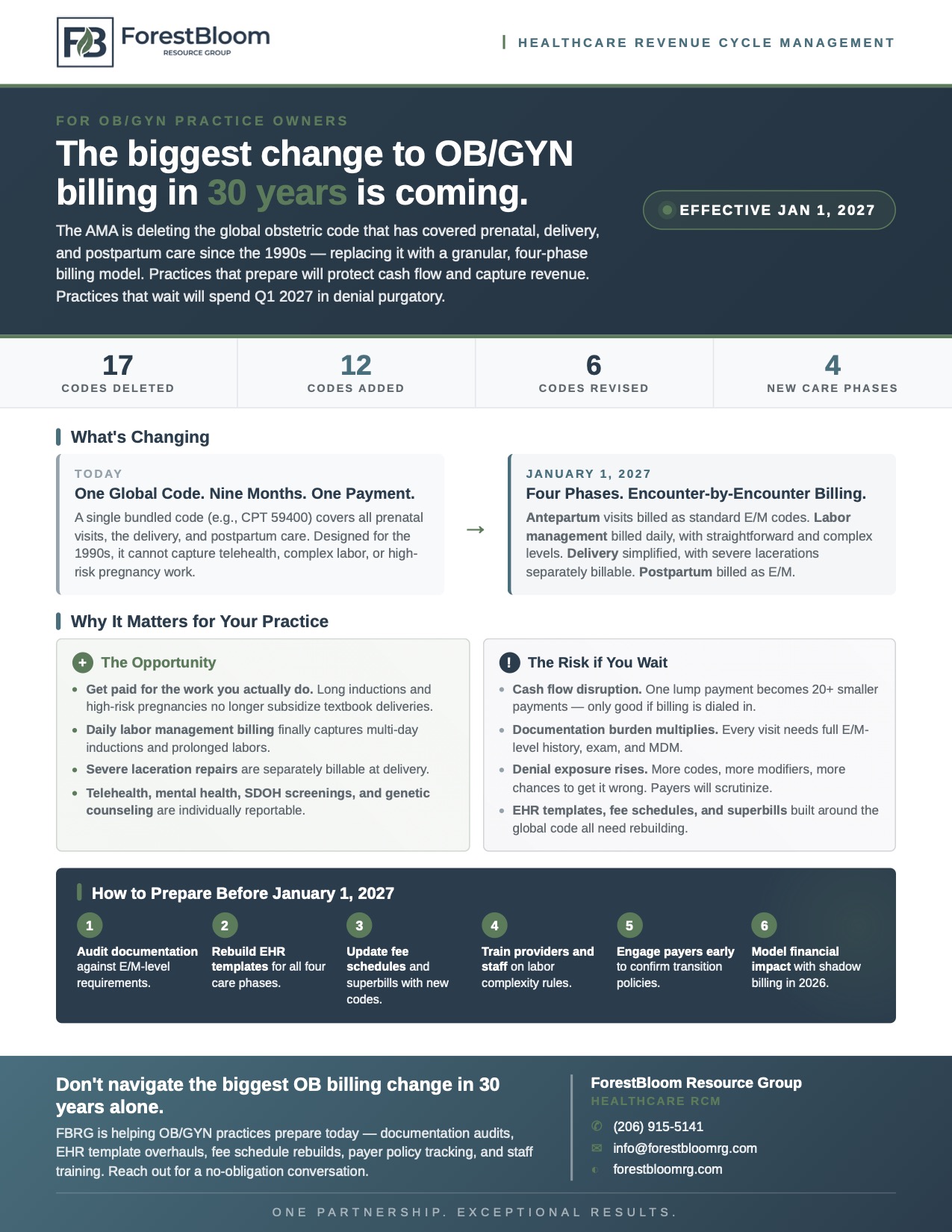
Effective January 1, 2027, the American Medical Association's CPT Editorial Panel is deleting 17 maternity care codes, adding 12 new codes, and revising 6 more — the most significant overhaul of OB/GYN billing in the lifetime of most practicing physicians. The familiar global package disappears, replaced by a four-phase, encounter-by-encounter billing model that mirrors how modern obstetric care is actually delivered.
For OB/GYN practice owners, this is both an opportunity and a hazard. Practices that prepare in 2026 will protect cash flow, capture revenue the old code never recognized, and emerge stronger. Practices that don't prepare will spend Q1 2027 in denial purgatory — submitting claims under codes that no longer exist, watching reimbursement stall, and discovering on the wrong side of a payer audit that their EHR templates and superbills are already obsolete.
This article walks through exactly what's changing, why it matters, and how to prepare.
How OB/GYN Billing Works Today
To understand the scale of the 2027 change, it helps to remember how the current system works.
Under the existing CPT framework, a routine vaginal delivery without complications has historically been billed under a single global code such as CPT 59400, which covers:
- All routine antepartum (prenatal) visits
- Admission to the hospital
- Management of labor
- The vaginal delivery itself
- Routine postpartum care, both inpatient and outpatient
Cesarean deliveries have been bundled similarly under CPT 59510, and vaginal birth after cesarean (VBAC) under CPT 59610. One code, one payment, nine months of work.
This bundled approach was elegant for the obstetric care of the 1990s. It is poorly suited to the obstetric care of the 2020s. Telehealth visits, mental health screenings, social determinants of health (SDOH) assessments, genetic counseling, and the management of high-risk pregnancies all sit outside what the global code was designed to capture. A practice managing a 32-hour induction with multiple complications has been reimbursed identically to one managing a textbook two-hour delivery.
The 2027 changes are the AMA's response to that mismatch.
What's Actually Changing on January 1, 2027
The new framework, published by the AMA's CPT Editorial Panel and effective January 1, 2027, restructures maternity care into four distinct phases, each billed independently:
- Antepartum care — billed using standard evaluation and management (E/M) codes
- Labor management — billed daily, with separate codes for straightforward and complex cases
- Delivery care — billed using new vaginal and cesarean delivery codes
- Postpartum care — billed using standard E/M codes
The 17 Deleted Codes
The deletion list includes the entire global obstetric package and its variants:
- CPT 59400 (routine global vaginal delivery) — deleted
- CPT 59409, 59410 (vaginal delivery only and with postpartum care) — deleted
- CPT 59425, 59426 (antepartum care, 4–6 visits and 7+ visits) — deleted
- CPT 59430 (postpartum care only) — deleted
- CPT 59510, 59514, 59515 (cesarean delivery global package and variants) — deleted
- CPT 59525 (subtotal/total hysterectomy after cesarean delivery) — deleted, mapped to a new code
- CPT 59610, 59612, 59614 (VBAC global package and variants) — deleted
- CPT 59618, 59620, 59622 (cesarean after attempted VBAC, global and variants) — deleted
- CPT 59050 (fetal monitoring by consulting physician) — deleted, replaced by a revised code
The 12 New Codes
The new code set introduces granular billing for labor management and delivery:
- 59080, 59081 — Initial day labor management, straightforward and complex
- 59082, 59083 — Subsequent day labor management, straightforward and complex
- 59431, 59432 — Vaginal delivery, with or without episiotomy; and after previous cesarean
- 59433, 59434 — Repair of third-degree and fourth-degree episiotomy or laceration
- 59502, 59503 — Cesarean delivery, primary and repeat
- 59504 — Subtotal or total hysterectomy after cesarean delivery
- 59623 — Uterine tamponade for postpartum hemorrhage management
The 6 Revised Codes
Six existing codes are being revised, including 59412 (external cephalic version), 59051 (fetal monitoring during labor by a consulting physician), 59414 (delivery of placenta only), 59300 (first- or second-degree laceration repair by a non-attending physician), and the unlisted procedure codes 59898 and 59899.
Why This Is the Biggest OB Billing Change in 30 Years
The mechanical changes — deletions, additions, revisions — understate the magnitude of what's happening. The conceptual shift is bigger than the code count suggests.
From Bundled to Itemized
Today, a practice submits one claim for an obstetric pregnancy. After January 1, 2027, that same pregnancy will generate something closer to 20 or more separate billable encounters: a series of antepartum E/M visits, one or more labor management days, a delivery code, and postpartum E/M visits. Every one of those encounters needs documentation that meets E/M coding standards on its own.
Labor Management Becomes Time-Sensitive — Sort Of
The new labor management codes (59080–59083) are reported once per calendar date and are stratified by complexity, not by hours. A 36-hour induction that crosses midnight is two reportable days; a 14-hour delivery in a single calendar date is one. The AMA explicitly notes that "the duration of labor does not indicate the complexity of labor management, unless prolonged labor is diagnosed." In other words: complexity is determined by maternal and fetal condition and the medical decision-making involved — not by the clock.
For practices that have absorbed the cost of long, complicated inductions under a single bundled fee for years, this is a structural revenue capture.
Severe Lacerations Become Separately Billable
Under the old model, third- and fourth-degree laceration repairs were absorbed into the global delivery fee. Under the new model, codes 59433 and 59434 are separately reportable when performed at the time of vaginal delivery. This is genuinely new revenue.
Telehealth and Ancillary Services Are No Longer Buried
Telehealth antepartum visits, virtual check-ins, mental health screenings, SDOH assessments, and genetic counseling — all of which existed in clinical practice but were buried inside a global code that didn't see them — are now individually reportable under their respective E/M and ancillary codes.
Where Practices Will Get Hurt If They Don't Prepare
The opportunity is real. So is the risk.
Cash flow disruption. A single $4,000 global payment becomes a sequence of 20+ smaller payments stretched across the pregnancy. If your billing operation is dialed in, total reimbursement can be equal or higher. If it isn't, you'll feel the gap immediately in Q1 2027.
Documentation burden multiplies. Every antepartum and postpartum visit now needs full E/M-level history, examination, and medical decision-making documentation. EHR templates built around the global code don't capture this. Providers who have been documenting briefly because "it's all in the global code" will need to change their habits.
Denial exposure rises. More codes mean more modifiers, more payer-specific edits, and more chances to get something wrong. Payers will scrutinize claims aggressively in 2027 as they adapt their own systems. Practices without a systematic denial management process will see their denial rates climb fast.
Operational artifacts need rebuilding. Superbills, fee schedules, EHR templates, and patient financial estimates were all built around the global code. All of it needs to be rebuilt before January 1, 2027 — not on January 1, 2027.
Payer policies are still being written. Commercial payers, Medicaid programs, and managed care organizations are still finalizing how they'll handle the transition. Some may continue accepting deleted codes during a grace period; others will not. Practices need to be tracking payer communications now and engaging contract managers directly.
A Six-Step Preparation Plan for 2026
Practices that treat this as a 2026 project will be ready. Practices that wait until November of next year will not. Here's the sequence we recommend:
1. Audit documentation against E/M-level requirements. Pull a sample of antepartum and postpartum visits from the last 90 days and ask: would this documentation support an E/M code on its own? If not, the gap is your starting point.
2. Rebuild EHR templates for all four care phases. Antepartum visit templates, labor management notes (with explicit fields for complexity indicators), delivery notes, and postpartum templates all need rework. Build them now, test them in 2026, refine them before go-live.
3. Update fee schedules and superbills with the new codes. Map every deleted code to its new replacement(s). Build the new codes into your billing system and verify they flow correctly through to claim generation.
4. Train providers and staff on labor complexity rules. The straightforward-versus-complex distinction in labor management (59080/81 vs. 59082/83) hinges on factors like multiple gestation, fetal monitoring abnormalities, prolonged labor stages, preeclampsia, severe maternal morbidity indicators, and previous cesarean. Providers need to document these explicitly when present.
5. Engage payers early to confirm transition policies. Reach out to your top commercial payers, Medicaid program, and any managed care organizations to confirm: their effective date, whether they'll accept deleted codes during a grace period, and any payer-specific guidance on the new labor management framework.
6. Model the financial impact with shadow billing in 2026. Take a representative sample of pregnancies completed in 2026 and bill them twice — once under the current global code, and once as if the new framework were already in effect. The variance is your forecast for Q1 2027 cash flow, and it tells you where to focus your preparation effort.
The Bottom Line
The 2027 maternity care overhaul is not a tweak. It is a structural change to how pregnancy gets paid for in the United States — and the practices that win will be the ones that treat 2026 as preparation time, not 2027 as adjustment time.
For OB/GYN practices already stretched thin on the operational side, this is exactly the kind of transition that benefits from outside expertise. Documentation audits, EHR template overhauls, fee schedule rebuilds, payer policy tracking, staff training, and shadow billing analyses are not work that can be slotted in alongside the day job of running a practice.
Forest Bloom Resource Group is helping OB/GYN practices prepare for the January 1, 2027 transition right now. If you'd like a no-obligation conversation about where your practice stands and what preparation will look like, we'd be glad to talk.
Sources: American Medical Association, CPT Editorial Panel — Maternity Care Services, effective January 1, 2027 (published in advance of the CPT 2027 Professional Edition). All CPT codes, descriptors, and guidelines are copyright American Medical Association.